
In an era where information is readily available and misinformation runs rampant, it can be challenging for healthcare providers to differentiate clinical facts from myths. Traditional continuing education (CE) strategies are inundated with evolving guidelines, varied expert opinions and widespread misinformation, often leading to suboptimal decision-making.
To directly confront this challenge, we created an educational format called Facts & Myths, which can easily be incorporated into any live or web-based educational program. The Facts & Myths format represents a deliberate shift in instructional design. It prioritizes identification of healthcare myths, self-reflection and active learning and is grounded in principles of adult learning. Data collected from two programs — one live and one web-based — highlights the applicability of this model to uncover knowledge gaps, shift attitudes and drive meaningful changes in clinical practice.
Execution of Facts & Myths in the Live Setting
At the live virtual 11th Annual Obesity Forum® webinar in the fall of 2023, the Facts & Myths format was delivered as an interactive segment designed to challenge misconceptions in obesity care and evaluate the accuracy of widely held beliefs related to key topics. Primary care providers (PCPs) were presented with five statements and asked to classify each as fact or myth. Their responses were immediately displayed and discussed in real time by expert faculty. Faculty commentary provided evidence-based information regarding whether the statement was true or false. This process was then repeated for the remaining obesity-related statements.
Execution of Facts & Myths in the Web Setting
The Facts & Myths format flows similarly in a web-based setting. However, it is important to note that interactive polling capabilities are required to obtain necessary data on the fact versus myth alignment. When a learner selects a statement as fact or myth, evidence-based information is provided, followed by a “bottom line” statement reflecting the true answer.
Results: Elucidating Areas of Misinformation
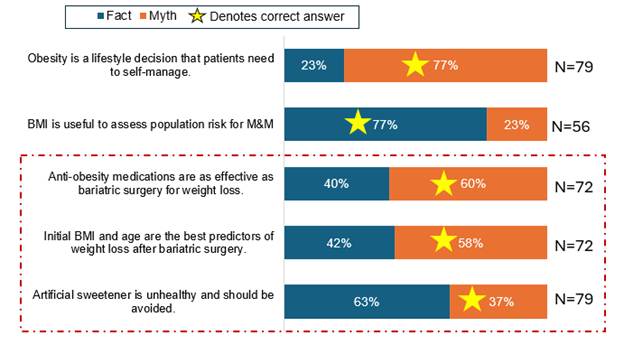
As shown in Figure 1, more than three-fourths of learners from the 11th Annual Obesity Forum® webinar recognized obesity as a disease and that body mass index (BMI) is useful to assess patient morbidity and mortality (M&M). However, misconceptions were observed regarding topics related to artificial sweeteners, predictors of post-surgical weight loss and comparative efficacy of anti-obesity medications (OMs) versus bariatric surgery, demonstrating areas of confusion and misinformation.
Figure 1 illustrates that 40% of learners erroneously believed OMs were as effective as bariatric surgery. At the time of the education in 2023, it should be noted that this statement was a myth, although the faculty indicated that OMs were quickly approaching the efficacy of bariatric surgery. Similarly, 42% misunderstood initial BMI and age to be the best predictors of response to weight loss after surgery. Finally, 63% misunderstood artificial sweeteners to be unhealthy, whereas, in reality, they can be a suitable alternative for individuals seeking to lose weight if used appropriately.
Figure 1: Learner Responses to Facts & Myths Statements in the Live Setting
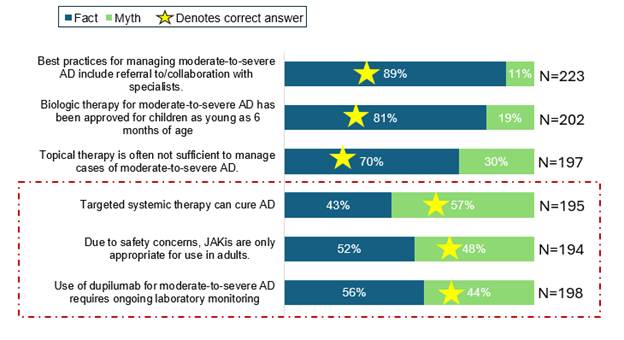
Similar insights can be garnered from execution of the Facts & Myths format in a web-based setting, as demonstrated in Figure 2. In this CE program about atopic dermatitis (AD) targeted to PCPs, understanding was observed regarding best practices to manage moderate-to-severe AD, the indication for biologic therapy to manage moderate-to-severe AD in pediatric patients, and use of topical therapy to manage patients with AD. Forty-three percent of learners falsely thought that systemic therapy could cure AD, 52% erroneously thought that Janus kinase inhibitors (JAKis) could be used only for adults, and 56% thought that laboratory monitoring was necessary for patients receiving dupilumab therapy.
Figure 2: Learner Responses to Facts & Myths Statements in the Web Setting
Results: Impact of Facts & Myths on Knowledge, Attitudes and Behaviors
The benefit of the Facts & Myths format in addressing knowledge gaps was evidenced by a 27% average knowledge gain across topics, ranging from a 9% increase on post-surgical predictors of weight loss to a 55% increase regarding appropriate monitoring of patients with AD receiving dupilumab.
From an attitudinal standpoint in the obesity program, PCPs were 8% more likely to recognize that OMs could help patients achieve weight loss goals and 19% more comfortable prescribing OMs post-learning. In the AD program (Figure 3), PCPs were on average 61% more comfortable with systemic treatment options post-learning. Aligned with this, 70% were highly confident in their ability to refer patients for systemic therapy.
Figure 3: Impact of Facts & Myths on Attitudes and Behaviors
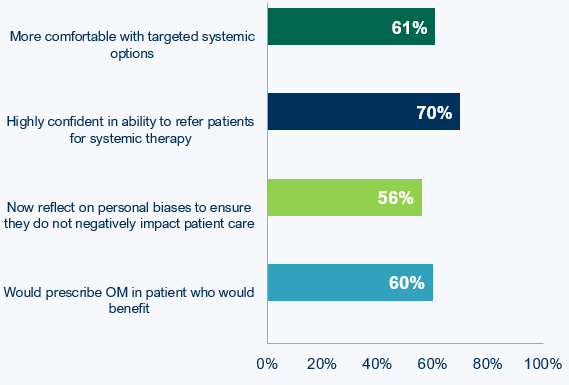
For the obesity program, which included a 30-day post-learning survey, 56% of learners indicated that they were now reflecting on their own personal biases and beliefs to ensure they do not negatively impact patient care (Figure 3). In addition, 60% would appropriately prescribe an OM for a patient who would benefit.
Discussion and Conclusion
The Facts & Myths CE format in both live and enduring settings has proven to be highly effective at uncovering common clinical misconceptions, facilitating targeted correction during the activity, and driving measurable post-learning impact on knowledge, confidence, and behaviors. Its success lies in engaging adult learners in active reflection and creating space for them to confront and revise outdated beliefs in real-time.
Whether delivered in a live or web-based environment, this format is rooted in myth-targeted polling questions and evidence-based expert debriefing. The development of each statement is informed by a comprehensive literature review, analysis of outcomes from previous educational programs, and expert faculty insights into current clinical debates. Purposeful faculty training, while minimal, is essential to success. Namely, faculty are briefed to moderate discussions in a reflective, nonjudgmental way, using polling data as a springboard to clarify misperceptions.
With a foundation in adult learning principles, this model equips clinicians to actively recognize and address misinformation and can be implemented using accessible strategies, such as real-time polling, engaged faculty, and carefully crafted statements designed to reflect clinical myths. Importantly, these basic strategies are not sophisticated CE tools, allowing for easy adaptation in a variety of educational settings. Although this article highlights primary care learners, the format is highly adaptable to interprofessional and specialty-specific education. Its structure can be customized for different clinical roles, with statements tailored to scope of practice and polling designed to foster cross-disciplinary dialogue.
In conclusion, the Facts & Myths format not only addresses myths in a real-time setting but can identify persisting areas of misinformation that can inform future CE programming. In addition, this format can be used to impact knowledge, attitudes and skills around misinformation to enhance patient care. Collectively, Facts & Myths has proven to be an engaging format to address misinformation, impact several levels of educational outcomes, and can be easily adopted to fit common educational settings, and tailored for interprofessional teams or specialty-specific audiences.
Disclaimer: The use of artificial intelligence is acceptable for Almanac publications. AI was used to improve the flow of the article.

Bharati Hegde, PhD, MS, currently serves as director, instructional design and analytics, at Vindico Medical Education. She applies her multidisciplinary background in biomedical engineering and content development to develop needs assessments and agendas for continuing education (CE) grants in various therapeutic areas. She is also involved in analyzing outcomes from prior CE activities and developing abstracts/publications for presentation at medical/industry conferences.
 Uniquely positioned within Vindico, Katie Robinson, PhD, CHCP, vice president, instructional design and analytics, applies her background in clinical pharmacology and basic science research to analyze outcomes from prior CE activities and identify gaps in provider knowledge and practice, using it to help mold the content and educational design of future programs. Actively involved within the CE community, Katie earned her CHCP designation in 2019 and serves as the editor-in-chief and chair of the Almanac Editorial Board.
Uniquely positioned within Vindico, Katie Robinson, PhD, CHCP, vice president, instructional design and analytics, applies her background in clinical pharmacology and basic science research to analyze outcomes from prior CE activities and identify gaps in provider knowledge and practice, using it to help mold the content and educational design of future programs. Actively involved within the CE community, Katie earned her CHCP designation in 2019 and serves as the editor-in-chief and chair of the Almanac Editorial Board.